THE EFFECT OF ANEMIA TO CARDIOVASCULAR RISK, LIPID PROFILE, AND GLUCOSE MONITORING IN PATIENT WITH TYPE 2 DIABETES MELLITUS IN SANGLAH GENERAL HOSPITAl
on
ISSN: 2303-2197
E-Jurnal Udayana Medica,vol 1 no 1 Januari 2017
THE EFFECT OF ANEMIA TO CARDIOVASCULAR RISK, LIPID PROFILE, AND GLUCOSE MONITORING IN PATIENT WITH TYPE 2 DIABETES MELLITUS IN SANGLAH GENERAL HOSPITAL
F. N. Anggreini1, G. P. Supadmanaba2, R. Saraswati2
ABSTRACT
1Medical Education Udayana University Medical School, 2Departement of Internal Medicine, Sanglah Hospital
Type 2 Diabetes Mellitus (T2DM) is chronic progressive disease which mainly marked by impairment of glucose utilization. Diabetic patients have high risk of anemia which is mainly caused by nephropathy with subsequent decreasing secretion of erythropoietin from renal medullar cells. A cross sectional analytic research was carried out to evaluate the prevalence of anemia among patients with T2DM and its correlation with CVD risk factors measured in medical record at Diabetes Centre of Sanglah General Hospital. The hemoglobin level, blood glucose concentration, HbA1c and lipid profile were collected and analyzed from 157 medical records as research sample which consist of 78 men and 79 women. The
frequency of anemia is found to be quite high, reaching 39.7% from all samples (cut off value, Hb=10g/dl). Anemia significantly
increased the risk of vascular complication by 8.143 times compare to non-anemic subjects with T2DM
(p=0.004). From this research is known that anemia in T2DM may have significant impact on evaluation, treatment adjustment,
mortality, and morbidity as well as precipitating CVD and accelerate progression of nephropati to ESRD which are major cause of mortality and morbidity in T2DM.
Keywords: type 2 diabetes mellitus, anemia, hemoglobin, cardiovascular disease.
Coresspondence :F.N Anggreini 1Medical Education Udayana University Medical School
INTRODUCTION
Type 2 Diabetes Mellitus (T2DM) is chronic progressive disease which mainly marked by impairment of glucose utilization. In the last 2 decade, T2DM has become pandemic and one of the major medical problems. In 2011, its prevalence reaches 346 million with rising trend parallel with obesity and metabolic
syndrome and projected to increase as much as 486 million in 2030.1 Complex pathogenesis in T2DM eventually leads to the emergence of various complications of T2DM.2 These include microvascular complications (i.e retinopathy, nephropathy), macrovascular complications (i.e atherosclerosis, peripheral artery disease), and neuropathic complication (Neuropathy).
Some complications such as ischemic heart disease and stroke have significant impact on diabetic survival, meanwhile the others like neuropathy and retinopathy mainly affect the quality of life. Despite enormous efforts to prevent such complications (lowering plasma glucose by oral hypoglycemic agent or insulin, improving lipid profile, and controlling hypertension), patient with T2DM eventually end up with at least one of them. In fact, most of T2DM patients have develop at least 2 complications at the first presentation.3
On the other hand, the prevalence of anemia in Indonesia is also very high, estimated to reach 50.6% which is mainly iron deficiency anemia. Because of its high prevalence, the likelihood of the cooccurrence of anemia and T2DM is also quite high. In fact, diabetic patients have high risk of anemia which is mainly caused by nephropathy with subsequent decreasing secretion of erythropoietin from renal medullar cells. The usage of metformin, the first line of oral hypoglycemic agent in T2DM management, is also predisposing factor of anemia because it depletes B12 storage by 30%. The other risk factors are diet pattern of diabetic patients which are commonly misinterpreted to avoid meat and gastropathy diabeticum. The occurrence of anemia in T2DM might have deleterious effect. Several studies in nondiabetic population had revealed that anemia is one of independent risk factors of cardiovascular disease (CVD) by decreasing oxygen supply to ischemic prone tissue distal to stenosed artery and also decreased the degree of obstruction needed to precipitated ischemia and tissue necrosis. Because majority of mortality and morbidity of T2DM are caused by CVD, it is likely that anemia had high potential to increase mortality and morbidity of patients with T2DM. Anemia is also proven to accelerate the
progression of nephropati. It may form a circle of morbidity where anemia accelerates progression of nephropati which will exacerbate anemia because of decrease secretion erithropoietin.
With so much progression in the knowledge about the relationship of anemia with CVD and renal disease, little is known about its effect on metabolic profile of diabetic patients. The basis of theory that underlies this problem is because effective metabolism of fat and glucose depend on oxygen supply which is correlate with level of hemoglobin. The level of HbA1C which is the main indicator of diabetic evaluation also depends on the level of hemoglobin. The correlation between hemoglobin level and lipid profile also poorly understood. One study shown there is inverse correlation between hemoglobin level and lipid profile component such as LDL, HDL, and triglyceride that might explain the low incidence of ischemic heart disease in population with mild anemia. So, it is interesting to evaluate the effect of anemia in T2DM especially its correlation with blood glucose level, HbA1c and lipid profile.
In this research, we examine the correlation between hemoglobin level with blood glucose concentration, HbA1c and lipid profile. We hypothesize there is correlation between hemoglobin level with metabolic profile of T2DM especially blood glucose, HbA1c, and lipid profile because of their metabolic dependence on oxygen. We hope that the result of this research will become the basis of future researches and become the basis of how will we consider the role of anemia in T2DM and the best way to manage it.
METHODS
This research is cross sectional analytic research which evaluates the prevalence of anemia among patients with T2DM and its correlation with CVD risk factors measured in medical record. Whole research process takes place in Sanglah General Hospital especially at Diabetes Centre for collecting the data from April 3rd - 24th 2012. This research use medical records collected at Diabetes Centre of Sanglah General Hospital.
Variables
The dependent variable of this research are anemia and hemoglobin level whereas the independent variable are systolic blood pressure and HbA1C. The operational definition of research variables are:
-
1. Anemia: Anemia can be define as hemoglobin level below normal value for sex, that is < 12g/dl for women and <14g/dl for men. According to National Cancer Institute, anemia can be classified into several categories8:
-
2. Cardiovascular Disease (CVD): Cardiovascular complication defined in this research include either macrovascular and microvascular complications like ischemic heart disease (IHD), ischemic stroke, heart failure, diabetic foot, retinopathy that recorded at patient’s medical record.
-
3. Hemoglobin A1C (HbA1C): HbA1C
readings were obtained from patient’s medical record. Glycemic control of the patients can be classified as good (HbA1C ≤6%), poor (HbA1C >6-9%), and worse (HbA1C >9%).
-
4. Fasting Plasma Glucose (FPG): FPG will be classified as normal (FPG<125 mg/dl) and high (FPG >125 mg/dl)
-
5. Two hours post prandial glucose concentration (2PPG): 2PPG can be
classified into <140 mg/dl, 140-199 mg/dl, and ≥200 mg/dl.
Sample
The target population in this research is patients at Sanglah General Hospital while researched population in this research is patients with T2DM at Sanglah General Hospital. Samples are calculated with this formula:
n = j^z^+3
{°≡'"⅛⅛)
With type I mistake that can be tolerated is decided to be 5% with one way hypothesis, so Zα = 1.64 and type II
mistake is decided to be 10%, so Zβ =
-
1. 28. Previous study showed that
relationship ratio between Hb and creatinine equals 0.4. So, the calculation should be:
_ J(l 64-123}3}
N --------I-D,] , 3
^5'"⅛^
V = 88
The minimum number of sample in this research is 88. To know whether this minimum number still meet the number of sample required for descriptive research, we use the formula:P XN > 5. With α = 5% and the prevalence of anemia in Indonesia 50,4%, the lower bound will be 45.4% × 88 = 40 and the upper bound will be 55.4% × 88 = 48.7. Because both of the values are > 5, the minimum number of the sample still meets the requirement for descriptive purpose.
The inclusion criteria in this research are medical records that being included in this
Table 1. Grading for anemia based on hemoglobin value
|
Grade |
Symptoms Severity |
Hemoglobin Value |
|
0 |
Within Normal Limits |
12.0-16.0g/dl for women 14.0-18.0g/dl for men |
|
1 |
Mild |
10.0g/dl to level within normal limits |
|
2 |
Moderate |
8.0-10.0g/dl |
|
3 |
Serious/Severe |
6.5-7.9g/dl |
|
4 |
Life Threatening |
<6.5g/dl |
Table 2. Characteristics of the samples and their normality
|
Variables |
Mean±SD |
Kolmogorov-smirnov test (p) |
|
Age |
55.6±11.4 years |
0.030 |
|
Body Mass Index (BMI) |
22.8±3.56 |
0.012 |
|
Systolic Blood Pressure (SBP) |
130.67±2.39 |
0.000 |
|
Hemoglobin Level |
10.85±2.5 g/dl |
0.200 |
|
Leukocyte |
13.67±8.5/dl |
0.000 |
|
Ureum |
27.18±2.43 mg/dl |
0.000 |
|
Creatinine |
1.93±2.48 mg/dl |
0.000 |
|
Total Cholesterol |
162.65±7.01 mg/dl |
0.200 |
|
Triglyceride (TG) |
146.24±1.04mg/dl |
0.000 |
|
HDL |
31.32±2.44 mg/dl |
0.000 |
|
LDL |
105.66±5.54 mg/dl |
0.200 |
|
Fasting Plasma Glucose (FPG) |
163.82±8.15 mg/dl |
0.004 |
|
Post Prandial Glucose (PPG) |
201.01±8.81 mg/dl |
0.021 |
|
HBA1c |
10.03±5.02 mg/dl |
0.000 |
|
SGOT |
36.2±4.66 mg/dl |
0.000 |
|
SGPT |
30.83±4.02 mg/dl |
0.000 |
research are those which belongs to patient with T2DM. The exclusion criteria in this research are medical records that being excluded from research which belongs to other types of diabetes, with incomplete data, from patient with bleeding or bleeding disorder, patient which is too old (>85 years), and had malignant disorder either solid tumor or hematological malignancy.
Research Procedure
Data Selection
Data of the patients are obtained from Diabetes Centre of Sanglah General Hospital. The data are selected based on inclusion and exclusion criteria. Then, baseline characteristic of the sample is analyzed by SPSS 16.
Evaluation of Subjects Baseline Characteristic and Prevalence of Anemia among Patients with T2DM
Baseline characteristic of the subjects (age, BMI, SBP, cholesterol, triglyceride, LDL, HDL, FPG, 2HPPG, and HbA1C) were obtained initially. Then, the prevalence of anemia is evaluated generally. Then the prevalence of each category of anemia is evaluated to know their proportion in diabetic patient’s population. Consider most of the anemia in diabetic patients is generally caused by nephropati, subjects were grouped into
group with serum creatinine <1.2mg/dl and gruop with serum creatinine >1.2mg/dl. Anemia is evaluated generally and specifically for each category.
Evaluation of Correlation between Hemoglobin Level with HbA1C
After prevalence of anemia had been assessed, the correlation of Hb with HbA1C was assessed. Before analyzing the correlation ratio, the normality of the data were assessed by Kolmogorov-Smirnov normality test. Then, the correlation ratio was assessed either by Pearson Correlation Test or Spearman’s Correlation Test depending on the result of normality test. The correlation between Hb and serum creatinine level was also assessed to confirm the correlation between anemia with renal function.
Data Analysis
Data analysis is conducted by using SPSS 16. The distribution of the data is evaluated by Kolmogorov-smirnov Test. The relationship between anemia and CVD is assessed by chi-square test. The correlation between Hb with glucose parameter was determined by Pearson or Spearman Correlation Statistic Method based on the result of Shapiro-Wilk Test.
RESULT
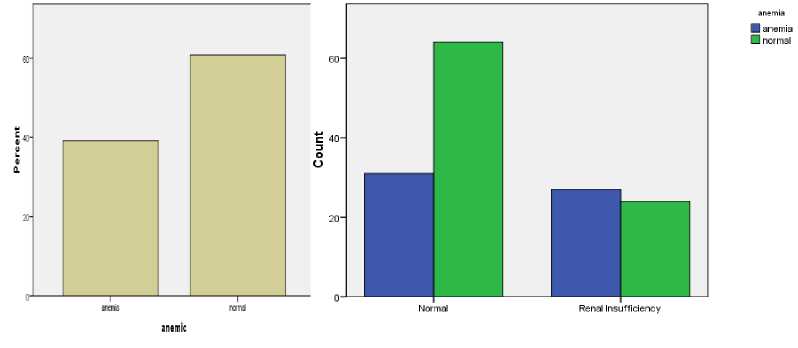
Figure 1. The frequency of anemia among patients with renal insufficiency compare to normal.
157 medical records are selected from 172 as research sample after excluding the inappropriate medical record based on exclusion criteria. The samples consist of 78 men and 79 women. Initially, baseline criteria and normality of the data were assessed. From all of the data being assessed, only hemoglobin, TG, and LDL that normally distributed (p=0.200). Baseline characteristics of the samples and their normality were described in table 2.
The frequency of anemia is found to be quite high, reaching 39.7% from all samples (cut off value: Hb=10g/dl). Most of the cases are mild and moderate anemia (24% and 28.1% respectively) but there are also a considerable number of samples with severe anemia (11.6%). Meanwhile, the frequency samples with elevated creatinine serum (cut off value = 1.2 mg/dl and classified as renal insufficiency) are as large as 34.9%. Since anemia in diabetic person most likely associated with renal disease, the frequency of anemia among patients with
renal insufficiency compare to normal one was assessed (figure 1). The result shows that the percentage of anemia in renal insufficiency group was higher than normal (50% in renal insufficiency group compare to 32.9% in normal group; p=0.041). But considerable number of patients in normal group also had anemia (32.9%).
Then we assessed the relationship between anemia and CVD. From all samples, we got the prevalence of vascular complication 49.7%. 62.2% of samples with anemia have vascular complication. The relationship between anemia and vascular complication become established after we assessed by chisquare test.
The result show significant relationship with chi-square value 8.073 (p=0.004) with PR=8.143 (p=0.004) which means anemia increase the risk of vascular complication by 8.143 times compare to non-anemic subjects.
Then we assessed the correlation between hemoglobin level, the parameter of anemia, with FPG, 2PPG, HbA1C, total cholesterol, HDL, LDL, and Triglyceride as the main risk factor of vascular disease and also the main targets of diabetes management and control (table 3). The relationship with creatinin serum was assessed in order to confirm the relationship between renal function and anemia which is the primary and widely confirmed cause of anemia in diabetes. From the analysis we found that hemoglobin level is negatively correlated with serum creatinine. Hemoglobin level was positively correlated with HbA1C but there is no significant correlation with FPG and 2PPG. Interestingly, hemoglobin level were also positively correlated with total cholesterol, HDL, and LDL but no significant correlation was found between Hb and TG.
Discussion
Anemia and T2DM are prevalent throughout the world as well as in Indonesia so it not surprising if they are overlapping. Complication of T2DM, nephropati, also one of cause of anemia.7 Because metabolic abnormality of T2DM
Table 3. The correlation between
hemoglobin level with FPG, 2PPG, HbA1C, total
cholesterol, HDL, LDL, and Triglyceride as the main risk factor of vascular disease among patient with T2DM
|
Variables |
Correlation Coefficient (r) |
p-value |
|
Serum |
-0.303 |
0.000 |
|
Creatinine | ||
|
Urea |
-0.273 |
0.001 |
|
Total |
0.277 |
0.002 |
|
Cholesterol | ||
|
HDl |
0.324 |
0.000 |
|
LDL |
0.361 |
0.000 |
|
HBA1c |
0.293 |
0.002 |
places the patients in high risk of cardiovascular and renal complication, it
is interesting to explore the exact correlation between hemoglobin level as parameter of anemia with other cardiovascular risk factors.
Previous studies explain that anemia in T2DM mainly caused by nephropati diabeticum.7 Apoptosis and fibrosis of renal interstitium lead to decrease secretion of erithropoietin, a hormon that regulate erithropoiesis in bone marrow secreted by renal interstitial cells mainly in renal medula. Low erithropoietin level slowing the erithropoiesis in bone marrow which ultimately lead to anemia of normocytic and normochromic type. Confirming the previous study and established theory, our finding also shown significant negative correlation between serum creatinine level with hemoglobin which may reflect the correlation between anemia with nephropati. Hemoglobin level also negatively correlate with ureum that also may relate with renal insufficiency. On the contrary, anemia also reported to accelerate the progression of renal insufficiency toward end stage renal disease (ESRD).6 So elevated serum creatinine may also reflect the progression of renal disease which is accelerate by anemia.
Interestingly, the prevalence of anemia also considerably high in patients with normal renal function (serum creatinine level < 1.2 mg/dl). This might indicate the presence of other causal factor of anemia in patients with T2DM. Some studies shows that serum erithropoietin level is decreasing even before the patient
9 experiencing nephropati.
Anemia in T2DM currently believes to relate to nephropati which cause decrease secretion of erithropoietin by cells in renal medulla.7 But several studies show other factors may also contribute as the cause of anemia in T2DM. The most apparent cause other than nephropati is vitamin B12 deficiency which is prevalent in elderly (in which T2DM tend to be more common). The deficiency might be caused by the diet because diet recommendation in T2DM tends to prohibit or lower meat consumption which is rich source of
vitamin B12 and iron. In addition, Indonesian diet that relies on rice as the main source of carbohydrate instead of whole wheat or fortified wheat may also increase the susceptibility of T2DM in Indonesia to vitamin B12 deficiency. The other factor that may cause vitamin B12 deficiency is metformin which is mainstay of treatment in T2DM. Several reports have been shows that prevalence of vitamin B12 deficiency in T2DM that use metformin range between 22-29% with possible deficiency reach around 52%. Metformin also has known to lower plasma vitamin B12 as much as 30%. The vitamin B12 deficiency may exacerbate the lowering secretion of erithropoietin in precipitating anemia in T2DM. Moreover vitamin B12 deficiency may also hasten neuropathy development in T2DM and increase cardiovascular risk because of elevation in plasma homocystein concentration. Meanwhile, in relation to diet recommended to patients with T2DM, iron deficiency might also possible risk factor but the evidence that support it still lacking.
Other possibility is anemia might be precipitated by inflammatory state of T2DM. In the last decade, metabolic induced inflammation has been proposed as precipitating cause of T2DM. Several cytokines such as TNF-α and IL-6 has been reported to be elevated in patients with T2DM and metabolic syndrome and have been known to be able to produce insulin resistance. On the other hand, these cytokines together with CRP has been reported to inversely correlate with serum iron and also may inhibit proliferation and differentiation of erythroid progenitor cells which result in anemia of chronic disease. Proinflammatory cytokines (mainly TNF-α) may also inhibit erythropoietin synthesis and secretion either directly or by accelerating the progression of nephropati. However, no significant correlation between leukocyte level with hemoglobin is found in this study.
Regardless of its cause, anemia may have negative impact on T2DM evaluation, treatment adjustment, morbidity and
mortality. In this study, we found significant positive correlation between hemoglobin with HBA1c meanwhile neither significant correlation is found between hemoglobin with FPG or PPG. This finding might have significant impact on T2DM evaluation that primarily relies on HBA1c. Low hemoglobin level in anemia may falsely decrease the concentration of HBA1c because the non-enzymatic glycation depend on both hemoglobin level and plasma glucose concentration. Thus, HBA1c that measure in patients with T2DM with anemia may lower than non-anemic T2DM patients with the same plasma glucose level. This will lead to failure of the clinicians to notice the need for treatment adjustment in such patients if the focus is on HBA1c without consideration in hemoglobin level, FPG and PPG. As result, T2DM progression will be accelerated with increased morbidity and mortality.
The impact of anemia in mortality and morbidity of T2DM mainly because anemia may precipitate CVD (either macrovascular disease or microvascular disease) and accelerate the progression of nephropati toward ESRD like previously mentioned. Because patients with T2DM supposedly develop atherosclerosis, low oxygen carrying capacity of the blood in anemia will decrease threshold that required to precipitate ischemia, distal to the stenosed artery. As previously reported, anemia is adverse prognostic factors in acute coronary syndromes (ACS) and heart failure. In addition, Atherosclerosis Risk in Community (ARIC) study also confirms that anemia is independent CVD outcome in community subject between ages 45 and 64 years. Moreover, anemia may also precipitate peripheral artery disease in T2DM with same mechanism as macrovascular disease.
On the contrary to previous findings, we also found that hemoglobin level was positively correlated with total cholesterol, HDL, and LDL but no correlation with TG which means anemic patients tend to have low level of total cholesterol, HDL, and LDL. This is seems
to have protective effect by lowering cardiovascular risk in anemic patients as mentioned by some studies. But those studies use non-diabetic population as the samples which have different metabolic profile than diabetic patients and thus, render its generalization on T2DM. Even if the same effect occurs in T2DM, the contribution of anemia in progression of renal disease will attenuate its beneficial effect toward lipid profile.
Anemia also reported to accelerate progression of nephropati to ESRD in T2DM. As previously reported, even mild anemia (Hb <13.8 g/dl) have profound effect on progression of renal disease possibly by enhancing fibrosis as a result from tissue hypoxia. As a result, the outcome of anemic patients with T2DM tends to be worse compare to non-anemic ones even if anemia is associated with low level of total cholesterol and LDL.
One key implication of this study is the importance of hematologic evaluation and intervention in patients T2DM since anemia is highly prevalent. Hemoglobin level must also take into consideration when evaluating patient with T2DM since it might falsely decrease HBA1c level in anemic patients. The regular evaluation of hemoglobin level and multivitamin supplementation in patients taking metformin might prevent the development of anemia in such patients. Evaluation of patient’s dietary pattern by nutritionist may also help to reduce risk of vitamin B12 and iron deficiency. Then, prevention of CVD and renal disease are strongly considered in T2DM patients with anemia since they are the major cause of mortality and morbidity in T2DM. At last, it needs further researches to evaluate the exact prevalence of anemia in T2DM population as well as to determine the risk factors associated with it. It also needs to be confirm the relationship between hemoglobin level with lipid profile because it might help to explain the low prevalence and incidence of CVD in mild and moderate anemia.
Despite of the finding, this study has several limitation that may take into
consideration like using secondary data and low number of samples despite higher than minimum number required (minimum samples required: 80).
Unavailability of data about patients diet may also take into account since it may help to determine the causal factors of anemia.
CONCLUSION
Anemia is prevalent in T2DM even in patients with normal kidney function. Hemoglobin as parameter of anemia has significantly negative correlation with serum creatinine and urea and positive correlation with total cholesterol, HDL, LDL, and HBA1c. Anemia in T2DM may have significant impact on evaluation, treatment adjustment, mortality and morbidity by obscuring HBA1c level and thus the adjustment of diabetic therapy as well as precipitating CVD and accelerate progression of nephropati to ESRD which are major cause of mortality and morbidity in T2DM. Taking hematologic evaluation (especially hemoglobin level) into consideration when evaluate the patients and addressing appropriate intervention as well as prevention to anemia will have beneficial effect to patients with T2DM.
REFERENCES
-
1. World Health organization.
Diabetes:Fast Fact 2011. Health statistics and informatics Department, World Health Organization, Geneva, Switzerland.
-
2. American Diabetes Association. 2011. Type 2 Diabetes Mellitus:Practical Target and Management. American Diabetes Association, Ney York, USA.
-
3. DeFronzo RA. Pathogenesis of Type 2 Diabetes Mellitus. Med Clin N AM 2004;88:787-835.
-
4. Oliva EN. A Review of General Management of Anemia. Am J Blood Res 2011;1(2):160-166.
-
5. Vlagopaulos, PT. Anemia as a Risk Factor for Cardiovascular Disease and All Cause of Mortality: The Impact of Chronic Kidney Disease. J Am Soc Nephrol 2005;16:3403-10.
-
6. Mohanram A, et.al. Anemia and endstage renal disease in patients with type 2 diabetes and nephropathy. Kidney International 2004;66:1131– 1138.
-
7. Vlagopaulos, PT. Anemia as a Risk Factor for Cardiovascular Disease and All Cause of Mortality: The Impact of Chronic Kidney Disease. J Am Soc Nephrol 2005;16:3403-10.
-
8. Bohlius J, et.al. Cancer-related
anemia and recombinant human
erythropoietin—an updated overview. Nature Clinical Practice
2006;3(3):152-164.
-
9. Fehr T. Interpretation of
erythropoietin levels in patients with various degrees of renal insufficiency and anemia. Kidney International 2004;66: 1206–1211.
Discussion and feedback