A TYPE OF DWARFISM FOUND IN SOUTH BENGKULU TO BE AN X-LINKAGE
on
JURNALBIOLOGI XI (2): 57-63
ISSN: 1410 5292
A TYPE OF DWARFISM FOUND IN SOUTH BENGKULU TO BE AN X-LINKAGE
choirul muslim*), bhakti karyadi**', aceng ruyani**), ice purnamawati**), hernani**' and sumiyati**)
Afiliation *): The Department of Biology, FMIPA Universitas Bengkulu)
**) The Department of Teaching Sciences, FKIP Universitas Bengkulu.
E-mail Address: milsumc@yahoo. com
ABSTRACT
We have reported here a specific human short stature population in Kedurang District, South Bengkulu. AH those are men, described as a mild dwarf (130-150 cm), detected after 5 to 10 years old, caused by the failure on lumbar backbone growth and development, and only found among the men. In this investigation, we examine the inheritance pattern of the dwarfism by using pedigree analysis, study the morphological comparison between the disorder and normal person, and finally we ascertain the variation among the disorder.
We accomplished a survey on pedigree family to at least 3-4 generations related to the disorder. The data are then tested with Chi-square test, and transformed to tree families and pedigree analysis. To investigate morphological performance and their variation, we collected morphometric measurements to both disorder and normal group of sample; they are the height, the vertebral bones length, head measurement, the leg and arm length (upper and fore side), and their indexes. The data were analyzed descriptively. To find out the variation, the quantitative expression and penetrance, we evaluated the data according to normal distribution with Z test.
The result showed all the dwarfisms in Kedurang are men, who inherited his gene from his carrier mother. As a result, the gene has tightly linked to X chromosome and supposedly belongs to Spondylo Epiphypeseal Dysplasia Tarda (SEDT). These were concluded from 32 related family of dwarfism. We found 19 dwarf persons, grouped into young, adult, and older persons. The their height were shorter than normal (136,5 cm), and the length of vertebrae was under normal value (51,5 cm). Their frontal extremity were shorter than the normal one, but they are in proportion with any part comprised them. Their feet were shorter, but the proportion of leg is longer than calf. The rest is as normally. Among the dwarf person, there are variations of the length. The phenotypic expressivity is varied in the vertebrae, leg, and calf; but the rest is relatively invariable. Their penetrance is strong, mostly in the height, length of vertebrae, and legs. Based on morphological data we concluded that the disorder in the Kedurang, South Bengkulu belongs to SEDT (Spondyloepiphyseal dysplasia tardd).
Keywords: short stature, lumbar backbone, dwarf x-linkage
INTRODUCTION
Achondroplasia is a morphological disorder triggered by 200 conditions leading to the growth and development failure of long bone maturity, and causes to dwarfism or short stature (Scott, 1996). The conditions belong to genetics as well as environmental factor(s). There are many different genes involve in the growth and development of long (epiphyseal) bone, including genes encode for bone materials mobilization during the growth and development, genes involves in the complex hormonal regulations, and their cellular as well as sub cellular signal transduction implicating in the regulation.
One of the known single autosomal allelic factor is a gene for protein FGFR3 (Fibroblast Growth Factor Receptor 3), responsible for the hormonal FGF3 (Fibroblast Growth FactorS) receptor protein located in the fibroblast cell membrane. The function of the protein is to receive FGF3 signal, and to control the in-activation of kinase, to stop the fibroblast division and eventually the fibroblast will undergo to cell maturity that is indicated
by the mobilization of bone material or ossification. The dominant mutan of FGFR3 will cause earlier inactivation of kinase without the control of FGF3. The conditions lead to the failure of the transduction, and the FGFR3 mutant will inactivate the fibroblast proliferation at premature steps of bone prolongation. Therefore, the long bone is undeveloped, and dwarfism is the final result. Heterozygote achondroplasia is a non lethal skeletal displasia, while the homozygote is mortal displasia (Francomano 2002).
Another type of dwarfism caused by the failure of vertebral back bone development is called Spondyloepiphyseal dysplasia (SED). The dwarf has a body-length in between 52-62 inches, or 132-157 cm. There are two types of SED; that are autosomal dominant Congenital Spondyloepiphyseal dysplasia (SEDC) and X chromosomal linkage Spondyloepiphyseal dysplasia tarda (SEDT).
Spondyloepiphyseal dysplasia tarda (SEDT)
The disorder Spondyloepiphyseal Dysplasia Tarda (SEDT) has been reported to have X chromosomal
Greek number is indicating generation number
Arabic number is indicating individual number
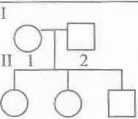
123
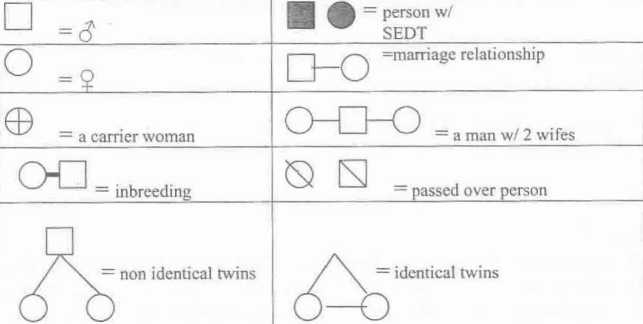
Picture 1. Symbols used in the pedigree tree analysis in this paper (Modified from
Suryo, 1997)
linkage (Gedeon et al, 2001), and described as mild dwarf (130-150 cm), exposed after 10 to 14 years old, caused by the failure on lumbar backbone growth and development, and only found among the men (Wilson, 2006). It is a heterogeneously expressed, and caused by the failure of epiphyseal growth and vertebral back bones, the trunk is comparatively short, a hunchbacked, enlarge chest, short neck, enlarge face, and the rest is as normally. In some cases the mature dwarf people also suffer from envision abnormality, and neural pain of the joint and spinal column (Wilson, 2006).
According to Gedeon et al (2001), SEDT in general have a medical condition on men rather than women, and it is because of the SEDT gene(s) is a recessive and tightly linked to X chromosome. The homozygote SEDT (X(S)X(S>) woman is theoretically lethal, while the heterozygote women is a carrier. The men, on the other hand, only have one X Chromosome (Apandi, 1992). As a result, the inheritance pattern of SEDT is a criss-cross inheritance (Wilson, 2006). A SEDT man will inherits his dwarf from his carrier mother, while the dwarf man will give his SEDT gene for his daughter.
The SEDT gene is located on lokus Xp22.2-p22.1 of X chromosome (Jang et al, 2002; Wilson, 2006). The gene is responsible for the protein(s) called TRAPP (^Transport protein particles), which have a specific role in the transport of protein to be exported extra-cellularly via endoplasmic reticulum and golgi vesicles. It is thought that the proteins involve in the mobilization of extra cellular materials'of fibroblast during the development of the vertebral back bones. Therefore, it is understandable when the SEDT or SEDL gene undergoes the mutation, it will result the malfunction of cellular transport of the cartilage protein. Although the specific mechanism
is still unidentified yet it is already acknowledged 4 different missenses mutation leading to the SEDT; they are three mutation (S73L, F83S, VI SOD) altering the protein structure, whereas another mutation (D47Y) is unsuccessfully establishing the functional interaction with a collaborative protein (Jang et al, 2002).
On our preliminary observation, we found such phenomena in Kedurang District, South Bengkulu. All those are men. We want to examine further whether the disorder belongs to the X chromosomal linkage, and to compare morphologically between the disorder and normal person, and finally to ascertain the variation among the disorder. Although this is only a kind of survey, we expected that our finding will give a picture of a scientific information regarding with the specific short stature in
Kedurang that will be employed as a
reference in the anticipation on how the suffer optimize himself to adapt into his/her
quality of life.
METHODOLOGY
Basically, the methodology we managed was a survey on pedigree family to at least 3-4 generations related to the disorder. It was conducted during September 2005 to April 2006 in the Kedurang district, South Bengkulu. The primary data (the dwarf family and their relations) collected from an interview to the correspondence. The data were the family and their members, the familial status of each person in the family, their names, sexes, morphological stature, and relation in the tree family. We also collected the secondary data associated with the demographic picture of the people living in the district. From the data, then we constructed a tree family and pedigree analysis, using the following symbols as in the box (picture 1).
Once we obtained the inheritance pattern from the pedigree tree, we examined the equivalent between inheritance data with the theoretical value using Chisquare test (Wier, 1996).
Finally, we collected morphometric measurements (in centimeters) to both disorder and normal group of sample with the purpose of investigate morphological performance and their variation; they are the height, vertebral bone length, head and chest measurement, leg and arm length (upper and fore side), and their indexes (%). The data were analyzed descriptively. To find out the variation, the quantitative expression and penetrance, we evaluated the data according to normal distribution
RESULTS AND DISCUSSION
We observed 8 existing families of short stature consisting of 32 persons in Kedurang. The families scattered in desa Rantau Sialang (1), desa Tanjung Alam (1), desa Nanti Agung 2 (2), desa Palak Siring (2), desa Nanti Agung 1 (1), and in desa Bumi Agung (1). After we examine the characteristics and analyzed the pedigree tree carefully, we suspected the dwarf belongs to a type called Spondyloephypeseal Dysplasia Tarda (SEDT) which has a thigh link to X chromosome.
In those families, we always found the case of dwarf man who born from a normal family, but his mother is carrier. The dwarf man get married with a normal woman, and their sons are normal. Those are typical in all pedigree trees, as observed.
Therefore, the characteristic inheritance in those families is always the followings: Parent (family 1)
H-6 (XSY), dwarf >< H-7 (XSXS), woman normal Fl
m XSY = men, 100% normal III (XSXS), carrier
As predicted, the dwarf is then showed up in the descendent grand sons, as indicated in the persons of IV-8 and rV-11 in the family 1 (see the pedigree tree). P (family 1)
m-15 XSY - men, normal >< 111-16 (XSXS), woman carrier Fl IV-10 XsY = men, normal
IV-8 and IV-11 (XSY), dwarf (IV-9) (XSXS), woman carrier
As typical in the family 1, this pattern is always the case in all the family, as it showed in the Table 1. It is clearly shown in the Table 1 that all the dwarf man inherited his SEDT gene from his carrier mother. The dwarf him self will not give rise a dwarf son, except to his grand-son. As a result, it is concluded that the dwarf belongs to a criss cross inheritance pattern and believed to be Spondyloephypeseal Dysplasia Tarda (SEDT) that caused by the mutation of SEDL gene located in the Xp22.2-p22.2 arm of X chromosomal as stated by Gedeon (2001). The disorders in Kedurang are only found among the men, short body height (least than 150 cm) and significant after 10 years old, with shorter neck, bend shoulder, wider chest, obverse maxilla, during infant age his capability to walk developed slowly, and they suffer from rheumatic at elderly age (Wilson, 2006; and Shotelersuk et al (1999).
In order to understand the reliability of the phenotype ratio, we test the data with
Chi-Square test (Wier, 1996). The Mowing Table 2 is the calculated data.
Calculated X2 = I (cfc/e) = 0,36 + 0,36 = (0,72). From
the value 0,72 and degree of freedom = 1, X2 table is located between value of 0,30 and 0,50 = ± 0,40. The calculated X2 > 0,05, so the observed data is suited with the theoretical value.
The probability of the dwarf be present
We calculated the proportion of dwarf from generation to generation, either at maternal or paternal lines. The results showed that the short stature is only found in the maternally line (see Table 3). As seen in the Table 3, the probability of having children with short stature is varied among the generation and among the family. The dwarf present in all generations we observed with 55% to 70% chance. The dwarf also present in all family ranging from 46 to 83 % chance. All those chance are observed in Table 3.
Phenotypic Morphological Comparison between dwarf and normal.
We found 19 persons with short stature, and this grouped into young (6 persons), 4 adult persons, and 9 older persons. Their height were shorter than normal (136,5 cm), and the length of their vertebrae reached 51,5 cm (under normal value). Their frontal extremity were short compare to the normal, but they are in proportion with any part comprised them. Their feet were shorter, but the proportion of leg is longer than calf. The rest is as normally.
The dwarf is sharply different with the normal people in terms of their height, vertebral length, front extremity, rear extremity, index of leg, and index of calf. In general orthogonal F test for the indicators) comparison between normal and short stature showed significant different. This means, that statistically the height of dwarf at young, adult, and elderlyare different with the ones in normal persons as indicated in Table 3. According to Scott et all, (1996) The SEDT skeletal displasia tend to have height of 51,8 inches or 129,5 cm. This met with what we observed, that is less than 150 cm (Gedeon et al, 2001, Wilson, (2006).
In order to understand the more comparative approach, here, we summarized in the Table 4 the Orthogonal F test to show the comparison between normal and dwarf in terms of some indicators. Here, again we saw that the main evident to distinguish the dwarf is vertebral length, body height, upper and lower extremity. Surprisingly, the index extremity is not distinguishable, and so are the measurement of head finger size, etc.
Phenotypic variation among the short stature
Among the person with short stature, the body height is varied. In terms of phenotypic expressivity, they are varied in the vertebrae, leg, and calf; but the rest is relatively invariable. Their penetrance are strong, mostly in the height, the length of vertebrae, and legs. This study takes a conclusion that the disorder in the Kedurang, South Bengkulu belongs to SEDT (Spondyloepiphyseal
Table 1, The pattern of marriage in the dwarfism family. Note that the dwarf is always born from a carrier mother, while the dwarf himself does not provide his gene to his son.
|
Family |
Parent |
Son and daughter | ||
|
Father DXSY |
n (carrier) XSXs |
Daughter XX |
Son XY 0 | |
|
1 |
II-6 XsY (dwarf) |
II-7 XSXS (normal) |
XSXs = normal carrier (111-16) |
XSY = laki-laki 100% normal |
|
111-1 5 XSY (normal) |
lll-16XSXs |
XSXs = normal carrier (IV-9) |
XSY, normal (IV-10), XsY, dwarf, (IV-8 dan IV-11) | |
|
2 |
111-11 (normal) |
111-1 2 (carrier) |
Normal : (IV-11, IV-12, IV-13) |
XsY Dwarf : (IV-8 and IV-9) |
|
Normal carrier (IV-7, IV-14) | ||||
|
IV-6 XSY (normal) |
IV-7 XSXs (carrier) |
XsY, dwarf = (V-8 dan V-9) | ||
|
3 |
I-8 XSY (normal) |
I-9 XSXs, (carrier) |
XSXs = normal carrier (II-8 11-16) |
XsY, dwarf = (II-9) |
|
4 |
I-6 XSY (normal) |
I-5 XSXs (carrier) |
XsY, dwarf (11-1 6 and 11-1 9) | |
|
5 |
II-8 XsY (dwarf) |
II-7 XSXS (normal) |
XSXs = normal carrier 1 00% (111-18,111-29,111-38) |
XSY = normal 100% |
|
111-17 XSY (normal) |
111-18 XSXs (carrier) |
XsY = dwarf IV-9, IV-13, IV-14, IV-15, IV-22, IV-38, IV-40, IV-44, IV-54, V-1 1 , V-46 and V-47) | ||
|
6 |
I-3 XsY (dwarf) |
1-1 8 XSXS (normal) |
XSXs normal carrier (11-5, 11-11, II-49, II-56, II-58) |
XSY, (all normal) |
|
1-10 XsY (dwarf) |
I-9 XSXS (normal) |
XSXs, normal carrier 1 00% (II-26, II-29, 11-31 , II-44, II-46) | ||
|
(normal) |
1-14 (carrier) |
Dwarf: II-40 | ||
|
Dwarf: II-40 |
11-41 (normal) |
normal |
normal | |
|
11-19, II-20, 11-21, II-26, II-27, II-29, II-44, II-50) | ||||
|
XSY (normal) |
XSXs (carrier) |
XsY = dwarf, (111-19, IM-20, 111-21, III-26, III-27, III-29, III-44, III-50, IV-36, dan IV-60) | ||
|
Normal |
(IV-41) |
Dwarf V-54 | ||
|
8 |
XSY (normal) |
XSXs (carrier) |
XSXs = normal carrier (III-2, III-4, III-65.III-93) |
111-7,111-14,111-91,111-94 |
|
XSY (normal) |
XSXs (carrier) |
IV-3, IV-8, IV-14, IV-87, IV-88, IV-103, I V-1 04 | ||
Table 2. The Chi-Square test for the phenotypic ratio of SEDT dwarf found in Kedurang.
|
Phenotype |
Observed |
Expected (e) |
D value |
(d2) |
(d2)/e |
|
Dwarf men |
53 |
40,5 |
3,85 |
14.82 |
0,36 |
|
Normal men |
28 |
40,5 |
-3,85 |
14,82 |
0,36 |
Table 3. The probability of having short stature at each generation in the family according to a matrilineal inheritance.
|
Generation |
Probability (%) of dwarf |
Family |
Probability (%) of dwarf |
|
1 |
55,55 |
1 |
60 |
|
II |
60 |
2 |
85,71 |
|
III |
62,98 |
3 |
46,15 |
|
IV |
69,69 |
4 |
83.33 |
|
V |
66,66 |
5 |
77,77 |
|
6 |
_ 60 | ||
|
7 |
56.52 | ||
|
8 |
63,63 |
dysplasia tardd).
Dwarf Height Variation. As shown in Table 5, the height among the young dwarf is on a range between 117 to 134 cm (young), 129 - 142 cm (adult dwarf), and 120 - 141 cm (elderly dwarf). Wilson (2006) stated that the height of SEDT dwarf is varied in between 130 to 155cm.
Dwarf Morphological Expressivity
Dwarf Morphological Expressivity on some of the indicators are summarized in the following Tables 6, Table 7, and Table 8. The data affirmed that there are variations among the indicators of dwarf at morphological
phenotypes level, implicating the interaction between gene expression and environmental modifiers. Perhaps, among the modifiers, nutrition is an important factor. The genetic constituent is a main predictor for the body height, and it is thought to be more than 50% comprise the height (Soetjiningsih, 2004).
The dwarf Penetrance
In table 9, it is shown that the penetrance of dwarf body height is 96,86% at young age, 100% at adult age, and 99,59% at elderly dwarf. It is a sign that almost dwarf persons are absolutely short in their stature. Furthermore, the observed penetrance are varied among different indicators.
The strongest penetrance (100%) occurs at height as indicated, followed by vertebral length, foot length, leg length. Whereas the least is at (4,01%) the index of fore-arm, followed by upper extremity, and head measurement. Again, the penetrancee value is an indication that the dwarf we found is confincingly belong to SEDT. (Gedeon et al, 2001; Wilson, 2006).
CONCLUSIONS
Based on the results and discussion above, we concluded that the dwarfism we found in Kedurang District South Bengkulu is a member of SEDT (Spondyloepiphyseal dysplasia tardd), that suspected to have X chromosomal linkage. The their height were shorter than normal (136.5 cm), and the length of their vertebrae
reached 51.5 cm (under normal value). Their frontal extremity were short compare to the normal, but they are in proportion with any part comprised them. Their feet were shorter, but the proportion of leg is longer than calf. The rest is as normally. Among the person with short stature, there are a variation of the length. In terms of phenotypic expressivity, they are varied in the vertebrae, leg, and calf; but the rest is relatively invariable. Their penetrance are strong, mostly in the height, the length of vertebrae, legs.
SUGGESTIONS
The above investigation was limited on exploring morphological data. Further DNA or protein examination need to be accomplished in order to ascertain precisely the dwarfism and to study variation in terms of molecular level.
At the same time, the disorder has led to rheumatic suffer. Perhaps, a medical research approach needs to be performed to facilitate an effort for the disorder persons reaching their healthy and wealthy live.
REFERENCE
Apandi, M. 1992. Dasar-dasar Genetika, Cetakan II (alih bahasa). Erlangga. Jakarta.
Francomano, C. 2002. Achondroplasia. http://www. Gene-clinies. Org/ profile/achondroplasia/defails. Html.
Gedeon, A.K., G.E. Tiller., M. L. Merrer., S. Heuertz., L. Tranebjaerg., D. Chitayat., S. Robertson., LA. Glass., R. Savarirayan., W. G. Cole., D. L. Rimoin., E.G. Kousseff., H. Ohashi., B. Zabel., A. Munnich, J. Gecz, and 1C. Mulley. 2001. The Molecular Basis of X-linked, Spondyloepiphyseal dysplasia Tarda. Am. J. Hum. Genet. 68:1386-1397.
Jang. S. B., Yoen-Gil Kim., Cho Yong-Soon., Sun Pann-Ghill., Kim yung-Hwa. dan
Oh Byung-Ha. 2002. Spondyloepiphyseal dysplasia Tarda. Journal of Biological Chemistry. Edisi 20 Desember.
Scott, C. I. 1996. Achondroplasia. By The Human Growth Foundation, http: //www. Ipaonline. Org.
Shotelersuk V; C. Ittiwut, S. Srivuthana, S. Wacharasindhu, S. Aroonparkmongkol,
A. Mutirangura, Y. Poovorawan. 1999. Clinical and Molecular Characteristic of Thai Patients with Achondroplasia. Department of Pediatrics, Faculty of Medicine, Chulalongkorn University. Bangkok. Thailand.
Soetjiningsih, S. 2004. Tumbuh Kembang Remaja dan Permasalahannya. Sagung Seto. Jakarta. 320
Suryo. 1997. Genetika Manusia. Gadjah Mada Universitas Press.Yogyakarta.
Wier, S.B. 1996. Genetic Data Analysis II (Methods For Discrete Population Genetic Data). Sinauer Associates, inc. Publisher Sunderland. Massachusets. Hal 19, 20 dan 27.
Wilson, F. J. 2006. Spondyloepiphyseal dysplasia. <http:// www. Ncbi. Nml. Nih. Gov/ Omim/ searchomim. Html>
Table 4. The summary of Orthogonal F test to show the comparison between normal and dwarf in term of some indicators.
4.1. Body Height
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average (cm) (X + Sdx) |
Range (cm) |
Average (cm) (X + Sdx) |
Range (cm) | |||
|
Young group |
12-15 |
3 |
124.3+6.82 |
118-130 |
147.5+1.85 |
142-152 |
|
16-18 |
3 |
128+10.28 |
117-134 |
160.5+2.62 |
152-164 | |
|
Older group |
19-30 |
4 |
136.5+5.93 |
129-142 |
165.6+1.58 |
162-169 |
|
Elder Group |
31-39 |
3 |
128.3+8.64 |
120-135 |
163.6+4.24 |
150-174 |
|
40-50 |
6 |
129 ±6.03 |
120-141 |
161.2±2.08 |
155-165 | |
4.2. Vertebral Length
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average (cm) (X ± Sdx) |
Range (cm) |
Average (cm) (X + Sdx) |
Range (cm) | |||
|
Young group |
12-15 |
3 |
45± 7.07 |
40-52 |
56.4+0.96 |
54-59 |
|
16-18 |
3 |
46.7+ 5.1 |
45-54 |
63.2+1 .3 |
61-68 | |
|
Older group |
19-30 |
4 |
51.5+5.4 |
45-57 |
66.1+1.91 |
61-73 |
|
Elder Group |
31-39 |
3 |
48.0+2.26 |
46-50 |
67.9+2.3 |
61-73 |
|
40-50 |
6 |
50.2+ 4.31 |
45-57 |
66.9±1.08 |
65-69 | |
4.3. Head circles
|
* Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average (cm) (X + Sdx) |
Range (cm) |
Average (cm) (X + Sdx) |
Range (cm) | |||
|
Young group |
12-15 |
53.77+ 2.85 |
51-56 |
54.2+0.77 |
57-56 | |
|
16-18 |
3 |
53.3+ 0.93 |
52-54 |
54.2+0.64 |
53-58 | |
|
Older group |
19-30 |
4 |
55.5±3.96 |
53-57 |
55.5+0.56 |
54-57 |
|
Elder Group |
31-39 |
3 |
53.67+2.85 |
51-56 |
55.1+0.9 |
54-58 |
|
40-50 |
6 |
54.33+2.19 |
50-57 |
55.4+0.68 |
54-57 | |
4.4. Upper extremity
|
Stage of development |
roup of age (years) |
Number of sample |
Group of dwarfism |
Group of normal | ||
|
Average (cm) (X ± Sdx) |
Range (cm) |
Average (cm) (X ± Sdx) |
Range (cm) | |||
|
Young group |
12-15 |
3 |
63.+ 1.13 |
62-64 |
64.1+1.48 |
59-66 |
|
16-18 |
3 |
63.+ 4.93 |
58-66 |
69.6±1.31 |
67-73 | |
|
Older group |
19-30 |
4 |
67.5+2.3 |
66-70 |
70.6+2.28 |
63-75 |
|
Elder Group |
31-39 |
3 |
65.004.93 |
60-68 |
71 .2+2.1 |
64-74 |
|
40-50 |
6 |
65.3+2.81 |
61-69 |
70.5+1.61 |
67-75 | |
4.5. Index of upper arm
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average |
Range |
Average |
Range | |||
|
Young group |
12-15 |
3 |
0.4.+ 0.01 |
0.38-0.42 |
0.39+0.01 |
0.38-0.42 |
|
16-18 |
3 |
0.39+ 0.00 |
0.40-0.40 |
0.40+0.00 |
0.390.42 | |
|
Older group |
19-30 |
4 |
0.39±0.02 |
0.39-0.42 |
0.41+0.01 |
0.38-0.44 |
|
Elder Group |
31-39 |
3 |
0.40+0.03 |
0.39-0.42 |
0.40+0.03 |
0-38-0.42 |
|
40-50 |
6 |
0.39+0.01 |
0.38-0.41 |
0.41+0.12 |
0.37-0.43 | |
4.6. Index of lower arm
|
Stage of development |
roup of age (years) |
Number of sample |
Group of dwarfism |
Group of normal | ||
|
Average |
Range |
Average |
Range | |||
|
Young group |
12-15 |
3 |
0.37+ 0.04 |
0.33-0.39 |
0.35±0.01 |
0.32-0.38 |
|
16-18 |
3 |
0.35+ 0.03 |
0.33-0.38 |
0.36+0.01 |
0.31-0.41 | |
|
Older group |
19-30 |
4 |
0.39+0.02 |
0.39-0.42 |
0.41+0.01 |
0.38-0.44 |
|
Elder Group |
31-39 |
3 |
0.36+0.03 |
0.33-0.35 |
0.35+0.01 |
0.32-0.38 |
|
40-50 |
6 |
0.36+0.02 |
0.33-0.38 |
0.36+0.02 |
0.33-0.37 | |
4.7. Index of arm finger.
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average |
Range |
Average |
Range | |||
|
Young group |
12-15 |
3 |
0.14.+ 0.01 |
0.13-0.15 |
0.14+0.01 |
0.12-0.15 |
|
16-18 |
3 |
0.13+0.02 |
0.12-0.14 |
0.13+0.01 |
0.12-1.15 | |
|
Older group |
19-30 |
4 |
0.13±0.01 |
0.11-0.14 |
0.13±0.00 |
0.12-0.15 |
|
Elder Group |
31-39 |
3 |
0.13±0.01 |
0.12-0.13 |
0.13+0.01 |
0.12-0.15 |
|
40-50 |
6 |
0.13+0.0 |
0.12-0.15 |
0.13+0.0 |
0.12-0.15 | |
4.8. Index of finger distance between mid finger and ring finger
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average |
Range |
Average |
Range | |||
|
Young group |
12-15 |
3 |
3.5.± 0.00 |
0 |
3.5.+ 0.00 |
0 |
|
16-18 |
3 |
3.5.+ 0.00 |
0 |
3.8.+ 0.1 6 |
3.5-4 | |
|
Older group |
19-30 |
4 |
3.3.+ 0.18 |
3.0-3.5 |
4.2.+ 0.16 |
4.0-4.5 |
|
Elder Group |
31-39 |
3 |
3.7.+ 0.33 |
3.5-4.0 |
4.2.+ 0.1 6 |
4.0-4.5 |
|
40-50 |
6 |
3.4.+ 0.1 8 |
3.1-3.5 |
4.2.+ 0.10 |
4.0-4.5 | |
4.9. Length of lower extremity
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average (cm) (X + Sdx) |
Range (cm) |
Average (cm) (X + Sdx) |
Range (cm) - | |||
|
Young group |
12-15 |
3 |
67.33.+ 5.70 |
62-72 |
77.5+1 .79 |
78-83 |
|
16-18 . |
3 |
69.+ 5.77 |
66-73 |
81.3±1.83 |
78-85 | |
|
Older group |
19-30 |
4 |
74.0+6.65 |
66-79 |
83.3+1 .00 |
80-86 |
|
Elder Group |
31-39 |
3 |
69.67±7.89 |
63-77 |
84.3+3.13 |
73-89 |
|
40-50 |
6 |
68.0+4.64 |
61-74 |
84.4±1 .91 |
72-87 | |
4.10 Index of leg
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average |
Range |
Average |
Range | |||
|
Young group |
12-15 |
3 |
0.55.+ 0.05 |
0.50-0.59 |
0.52±0.03 |
0.50-0.53 |
|
16-18 |
3 |
0.60+ 0.03 |
0.56-0.62 |
0.52+0.02 |
0.50-0.54 | |
|
Older group |
19-30 |
4 |
0.55+0.02 |
0.52-0.57 |
0.52+0.00 |
0.51-0.53 |
|
Elder Group |
31-39 |
3 |
0.54+0.03 |
0.53-0.57 |
0.52±0.00 |
0.51-0.55 |
|
40-50 |
6 |
0.55+0.02 |
0.53-0.58 |
0.52+0.05 |
0.51-0.53 | |
A Type ofDwarfism Found in South Bengkulu to Be An X-linkage [Choirul Muslim, dkk.]
4.11. Index of Calf.
|
Stage of development |
roup of age (years) |
number of sample |
Group of dwarfism |
Group of normal | ||
|
Average |
Range |
Average |
Range | |||
|
Young group |
12-15 |
3 |
0.45. + 0.04 |
0.41-0.48 |
0.46+0.01 |
0.44-0.49 |
|
16-18 |
3 |
0.44+ 0.00 |
0 |
0.45+0.00 |
0.47-0.49 | |
|
Older group |
19-30 |
4 |
0.46+0.03 |
0.41-0.48 |
0.48+0.01 |
0.45-0.49 |
|
Elder Group |
31-39 |
3 |
0.46+0.03 |
0.44-0.48 |
0.48+0.01 |
0.45-0.49 |
|
40-50 |
6 |
0.45+0.02 |
0.42-0.48 |
0.48+0.01 |
0.47-0.49 | |
*) = Significant different
**) = highly significant different
NS or no sign = no significat different
Table 5. Phenotypic variation among the short stature
|
Phenotypic Indicator |
Young Dwarf |
Adult Dwarf |
Elderly (old) Dwarf |
|
Height variation (cm) |
117 to 134, or 126,167 ± 7,414 |
129 to 142, or 136,5 ± 5,447 cm |
120-1 41, or 128,779 ±7,759 |
|
Vertebral length (cm) |
40 s/d 54, or 47,333 ± 5,502 |
45 s/d 57, or 51 ,5 ±5,508 |
45 s/d 57, or 49,444 ± 4,503 |
|
Head measurement (cm) |
51-56, or 53,333 ±1,751 |
53 s/d 57, or 55,50 ± 1 ,732 |
50 s/d 57, or 54,111 ±2,522 |
|
Foot length extremity (cm) |
62-73, or 68, 167 ±4,021. |
70-79, or 74 ±3,91 6 |
61-77, or 68,556 ± 5,833 |
|
Calf-leg index (%) |
0,412-0,484, or 0,445 ± 0,024 . |
0,414-0,481 , or 0,455 ± 0,032 |
0,423-0,476, or 0,456 ± 0,019 |
|
Hand extremity (cm) |
58-66, or 63 ± 2,828 |
66-70, or 67,5 ±1,91 5 |
60-69, or 67,5 ± 3,28 cm |
|
Finger size (cm) |
8,5 ± 0,548 |
8,75 ± 0,5 |
8,556 ± 0,527 |
63
Discussion and feedback