CHARACTERISTICS OF AMBLIOPIA IN ANISOMETROPIC PATIENTS AT EYE POLYLINIC SANGLAH GENERAL HOSPITAL DENPASAR
on
Journal of Health Sciences and Medicine, Vol. 2 No. 1, February 2018
CHARACTERISTICS OF AMBLIOPIA
IN ANISOMETROPIC PATIENTS AT
EYE POLYLINIC SANGLAH GENERAL
HOSPITAL DENPASAR
Ni Putu Pradita Dhriti Indriyani Sukadana1, Ni Ketut Niti Susila2, Putu Budhiastra2, Ariesanti Tri Handayani2
1Medical Doctor, Faculty of Medicine, Udayana University Denpasar Bali-Indonesia 2Department of Ophthalmology, Faculty of Medicine, Udayana University Denpasar Bali-Indonesia Email: praditadhriti@gmail.com
ABSTRACT
The purpose of this cross sectional study was to determine the characteristics of amblyopia in anisometropic patients at Eye Polyclinic Sanglah General Hospital Denpasar.The data hat obtained are secondary data derived from medical records of refractive error in anisometropic patients on April 2016-August 2017 period, and involved 62 patients as research subjects based on consecutive sampling.The results of this study showed that from 62 anisometropic patients, there were 56 patients (90%) affected amblyopia. Based on the sociodemographic aspect, the highest number of patients with amblyopia in the children age group were 24 peoples (43%), females more than males were 37 peoples (66%), the majority of patients living in Denpasar were 28 peoples (50%), and the students were the most type of occupationin amblyopic patients is 35 peoples (63%). Patients with severe anisometropia were 24 peoples (43%), moderate amblyopia at 48 eyes (43%), and affected on both eyes (ocular dextra sinistra) about 35 peoples (63%). The type of refractive error was found to be at most is astigmatism about 74 eyes (66%), and the use of spectacles in 51 people (91%).Based on this research, it can be concluded that subject who were affected amblyopia in anisometropic patients most at age children, female, living in Denpasar, and as students. Severe anisometropia, moderate amblyopia, affected on both eyes, astigmatism, and the uses of spectacles were found to be the most of the subject.
Keywords:Amblyopia, Anisometropia, Refractive Error, Descriptive
-
I. INTRODUCTION
Ambliopia (lazy eye) is defined as a decrease in vision ability on one or both eyes which not caused by optical or retinal disorders. It may also be defined as a visual impairment system that characterized by a decrease in the best correction visual aquity of the eye without any organic pathology.1,2 Ambliopia is caused by a history of abnormal vision in the early stages of life caused by one of the following: refractive errors between the two disparate eyes (anisometropia), higih refractive errors between two eyes (isometropia), strabismus, and lack of stimulus.1 Anisometropia is a visual disturbance due to the difference in refractory power of the spherical lens or cylinder between the right eye and the left eye. Common symptoms arise in anisometropia is blurred vision due to refractive abnormalities, tired eyes accompanied by
headache. The most common problems caused by anisometropia are amblyopia and strabismus. Data of Optometry in Practice3, states that the limits of refraction strength in the eyes of myopia, hypermethropia, and astigmatism that can cause amblyopia are more than 2.00D, 1.00D and 1.50D, respectively, whereas according to Ilmu Penyakit Mata limit of refraction difference of more than 2.50D.4 Increased degree of anisometropia in both myopia and hypermetropia, can increase the incidence and degree of amblyopia severity, as well as astigmatism of myopia and hypermetropia of more than 1.50D will also increase the risk of amblyopia and its severity and decrease binocular vision (p = 0.05).5
In Indonesia study on the prevalence of amblyopia has been done in grade 1 elementary school in Bandung Municipality of 1.56% in 1989,6 in Yogyakarta (DIY) on 2005 by 0.32% from 54,260 elementary school students in 13 sub-districts,7 whereas in 2008 it was 1.5% of 2,268
elementary school students aged 7-13 years. The most common cause of amblyopia in the study was anisometropia of 44.4%.7,8
In Bali the number of patients visiting the hospitals in 2014 with complaints of refraction disorders as many as 6,615 people.9 But so far, there has been no research data on characteristics of amblyopia especially in anisometropic patients at Sanglah General Hospital (RSUP) Denpasar, so it is necessary to do research to know the characteristics of amblyopia in anisometropic patients in Bali, especially in RSUP Sanglah, Denpasar.
-
II. METHOD AND PROCEDURE
The type of this research is descriptive research with cross sectional approach. The study was conducted on medical records of patients with refractive disorders with anisometropia who experienced amblyopia in the Medical Record and Eye Polyclinic Sanglah Hospital, Denpasar. Calculation of the sample size using the formula need minimum number of samples, ie a number of 25 people. The samples used were those that met the inclusion and exclusion criteria, which were taken through the consecutive sampling method. The data obtained are then analyzed and presented in the form of tables and diagrams.
-
III. RESULT AND DISCUSSION
Based on patient registers data from April 2016 until August 2017, 62 subjects who meet the inclusion criteria were selected. Subjects who have met the inclusion criteria are then performed a scanning, then found only 56 people who experience amblyopia. Based on sociodemography factor, frequency distribution, and percentage of amblyopia patients as shown in Table 1 below :
Table 1.
Frequency Distribution and Percentage of Amblyopia Patients Based on Sociodemography
|
Sociodemography |
Frequency |
Percentage (%) |
|
Age (years) | ||
|
Children (4-11) |
24 |
43 |
|
teens (12-25) |
15 |
27 |
|
adult (26-45) |
5 |
9 |
|
Old age (46->65) |
12 |
21 |
|
Total |
56 |
100 |
|
Gender |
Frequency |
Percentage (%) |
|
Male |
19 |
34 |
|
Female |
37 |
66 |
|
Total |
56 |
100 |
|
Region |
Frequency |
Percentage (%) |
|
Denpasar |
28 |
50 |
|
Badung |
8 |
14 |
|
Gianyar |
4 |
7 |
|
Klungkung |
3 |
5 |
|
Bangli |
2 |
4 |
|
Karangasem |
5 |
9 |
|
Buleleng |
2 |
4 |
|
Jembrana |
3 |
5 |
|
Luar Bali |
1 |
2 |
|
Total |
56 |
100 |
|
Employment |
Frequen cy |
Percentage (%) |
|
Student |
35 |
63 |
|
Government employees |
4 |
7 |
|
Private employees |
7 |
13 |
|
Entrepreneur |
1 |
2 |
|
Housewife |
3 |
5 |
|
Not working |
6 |
11 |
|
Total |
56 |
100 |
Table 1 shows anisometropic patients with amblyopia dominated by the age group of children (4-11 years) and a seemingly decreased the distribution in the adult age group. This decrease is likely due to the chance of development to get amblyopia in adulthood was very small.10The age distribution of this study is similar to the reported of Woldeyes11 which the age distribution of patients is highest in the 4-10 years age group (72.8%), and Alarape et al.12 with the highest distribution in the 5- 9 years (50%), while Siddiqui et al.13 reported that distribution in the age group of 10-20 years as equal as 21-20 years. The difference in the results of this study with some other studies is due to the differences in age range of each category. Theoritically, amblyopia can develop in the critical period of the process developing of vision at the age of 6-8 years. If during this critical period one or both eyes do not receive any adequate visual sensitization, it will lead to be failure of the normal development of the visual pathway.14,15
The majority of samples in this study showed a higher ratios in female than male (66%). Alarape et al.12 reported that the gender distribution of amblyopic patients in most anisometropia was female (70%). Different results also reported by Woldeyes11 and Siddiqui et al.13 where males were the mostly found of 72.7% and 60%. Differences
result can be occur, because literary sources had mention that the development of amblyopia is not influenced by gender differences.15
In this study the majority of patients live in Denpasar (50%). This can be founddue to the location of Sanglah Hospital that located in the center of Denpasar city. These results can also serve as the main target in doing eyes screening in the community. Students were most likely to had ambliopia (63%), it is due to the majority of this study sample were children and adolescents aged students. However, other study had reported that there was no statistically significant association between amblyopia and occupational classification was found.16,17
The frequency distribution and percentage of patients with Amblyopia when seen from the degree of Anisometropia are shown in Figure 1 below.
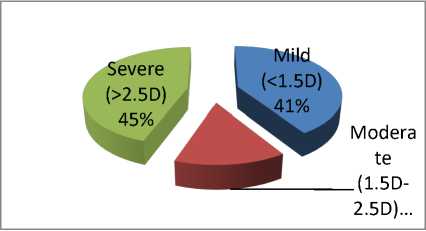
Figure 1. Frequency Distribution and Percentage of Amblyopia Patients
based on the degree of Anisometropia
Based on the results of this study, it was found that patients with amblyopia were distributed as equal as patients with refractive errorsin mild degree anisometropia (41%) and severe degree (45%), as shown in Figure 1. In this study also known that the occurrence of amblyopia in anisometropicpatients as much as 90%. Similar results also reported by Basyir18that were conducted in Kariadi Hospital Semarang, which the frequency distribution of anisometropia was found mostly on the severe degree, ie 14 people (50%) while mild degree ie 12 people (42.8%). However, different study were reported by Kuswandari5which is mild degree of anisometropia was found to be the most (80.6%). The degree or severity of anisometropia is associated with an increase in amblyopia severity.5,19 The incidence of amblyopia due to anisometropia was higher than subjects without anisometropia of 56.7%.20 This result is supported by a study conducted by Widadi21 who reported that anisometropia has 13 times risk to be develop as amblyopiabased on statistical test results. Other study were conducted by Chia et. al22 showed that anisometropia was the most common cause of patients with amblyopia (78.3%). Several
studies have also shown anisometropia as the most common cause of amblyopia.13,23,24,25,26
The degree or severity ofamblyopic patientsare most distributed to moderate degree which was 48 (43%), followed by mild degree of 29 eyes (26%), and severedegree of 14 eyes (13%) as shown in Figure 2.
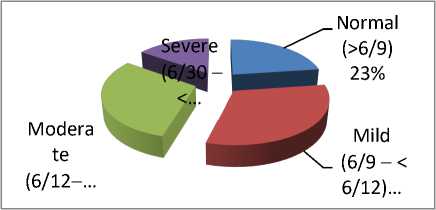
Figure 2. Frequency Distribution and Percentage of Amblyopia Patients based on Amblyopia Degree
Pediatric Eye Disease Investigator Group27also conducted a study of amblyopia degree of patients with anisometropia, which the most
distribution results at moderate degree (58%). Waris28 and Woldeyes11 also reported similar results where the highest frequency distributions in moderate degree were 53% and 54.5% respectively. But unlike the study conducted by Bhandari29, the frequency distribution is almost evenly distributed in moderate amblyopia ie 35.2% and
severeamblyopia 38.3%. Differences in the frequency distribution which reported by some researchers may be due to the presence of refraction error that chronically degrade the quality of shadow formations in the retina during early developmental as the cause of amblyopia. Increased degree of anisometropia in both myopia, hypermethropia, and astigmatism of myopia and hypermethropia may increase the incidence and severity of amblyopia.5,28,30 A significant amount of amblyopia severity is also affected by the severity of the ambliogenic factor, delayedof the patient in performing the examination, and the improper management of amblyopia.29
The most frequency distribution of eyes involvement in amblyopic patientswere in the ocular dextra sinistra (ODS) ie 35 persons (63%) or
70 eyes, as shown in Figure 3 below.
Ocula
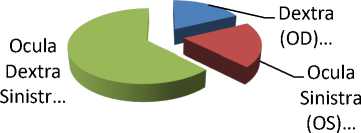
Figure 3. Frequency Distribution and Percentage of Amblyopia Patientsbased on Eye Engagement
Similar results were reported by Alarape12, which the most frequency distribution at ocular dextra sinistra (bilateral) is 54.4% and Gupta25 with the most frequency distribution were 58.06%. Several studies of eye involvement with amblyopia and dominated by ocular sinistra or unilateral amblyopia have been reported by Woldeyes11, Marthala31, and Repka et al.32. However, study that conducted by Goh et al.33 and Robaei et al.20 reported that the difference of involvement between the right and left eye on the occurrence of amblyopia was not statistically significant. The literature sources suggest that amblyopia may occur on one (unilateral) or both (bilateral), but more common in one eye.1,19 Bilateral amblyopia or the involvement of both eyes is associated with a severe refraction error of astigmatism or hypertropia in both eyes.34,35 In this study, the research samples obtained more on refraction disorders with astigmatism in both eyes, due to the involvement of the eyes of the patients in the oculardextra sinistra (bilateral).
Refractive disorders as the most distributed cause of amblyopia in astigmatism were 74 eyes (66%), which consisting of astigmatism myopia of 66 eyes (59%) and astigmatism hipermetropia of 8 eyes (7%). Patients with simplex myopia were 28 eyes (25%), and the lowest distribution in
hypermethropia was 6 eyes (5%) as shown in
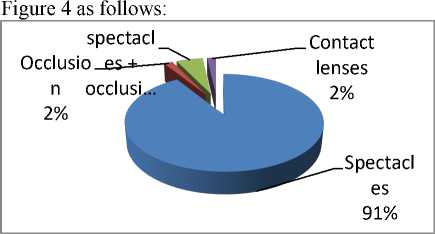
Figure 5. Frequency Distribution and Percentage of Amblyopia Patients
based on Therapeutic Choice
Early therapeutic in anisometropicamblyopia is the optimal correction of refractory disorders using spectacles or contact lenses with cycloplegi.40,41Intervention research conducted by Wallace et al.42, reported that the most therapy given to patients by only using spectacles with 88%. In Bhandari et al.29 study at Bharatpur Eye Hospital, 50% of samples were used ofspectacles and 8% received occlusion therapy using patching. On the use of spectacles, patient compliance rates are reported to be excellent, as well as high improvements in vision can be achieved well.42 The occlusion of the eye with patching is done very well in children because it can improve the improvement of vision. According to Stewart et al.43, therapy with occlusion provides better results
in children under 4 years of age. However, the patient's compliance level and the patient's companion whiledoing the therapy still low.40
-
IV. CONCLUSION
Characteristics of amblyopia patients in anisometropia is dominated by the age group of children and female sex. Severe anisometropia, moderate amblyopia, concerning both eyes, astigmatism, and use of glasses were most prevalent in the subjects studied.
REFERENCES
-
[1] Huang CB, Zhou J, Lu ZL, dan Zhou Y.
2011. Deficient binocular combination reveals mechanisms of anisometropic amblyopia: Signal attenuation and interocular inhibition. Journal of Vision (2011) 11(6):4, pp.1–17
-
[2] Lee CE., Lee YC., Less SY. 2010. Factors Influencing the Prevalence of Amblyopia in Children with Anisometropia. Korean J Ophthalmol 2010;24(4; pp.225-229
-
[3] Simmers AJ, Dulley P. 2014. Amblyopia and the Relevance of Uncorrected
Refractive Error in Childhood. Optometry in Practice Vol 15 (4).
-
[4] Ilyas S. 2006. Kelainan Refraksi dan
Kacamata. Jakarta: Balai Penerbit FKUI
-
[5] Kuswandari Y dan Ali HM. 2007.
Hubungan Antara Besarnya Ambliopia dengan Kedalaman Penglihatan Binokuler dan Ambliopia pada Anak Usia Sekolah di Unit Rawat Jalan Mata RSU dr. Soetomo Surabaya. Jurnal Oftalmologi Indonesia Vol.
-
5, No.1.; pp.58-64
-
[6] Sastraprawira R. 1989. Prevalensi Ambliopia pada Murid Kelas I Sekolah Dasar di Kota Madya Bandung. Bandung. Tesis; pp.4-9
-
[7] Triyanto W. 2006. Ambliopia pada Anak Sekolah Dasar dengan Kelainan Refraksi di Daerah Istimewa Yogyakarta. Tesis.
-
[8] Suhardjo S, MB.; Anugrahsari S. 2008. The Yogyakarta Eye Study: A Pilot Assessment of Astigmatism and Amblyopia in Elementary School Children. Clinical and Experimental Ophthalmology 2008; 36 (Supp I): pp.A278-A281.
-
[9] Dinas Kesehatan (Dinkes). 2015. Profil Kesehatan Dinas Kesehatan Provinsi Bali Tahun 2014. Bali: Dinas Kesehatan Provinsi Bali
-
[10] American Optometric Association (AOA).
2017. Amblyopia FAQs: Who is likely to develop amblyopia? Tersedia pada: https://www.aoa.org/patients-and-
public/eye-and-vision-problems/glossary-of-eye-and-vision-
conditions/amblyopia/amblyopia-faqs. [22]
[diunduh 30 November 2017]
-
[11] Woldeyes A, dan Girma A. 2008. Profile of
Amblyopia at the Pediatric Ophthalmology Clinic of Menilik II Hospital, Addis Ababa.
Ethiop.J.Health Dev.; 22(2)
-
[12] Alarape AT, Ulaikere M, Okoye O, [23]
Okonkwo O, Mahmoud AO, Nwachukwu
N, et al. 2017. Burden and Spectrum of
Amblyopia in a Pediatric Hospital
Population Southwest Nigeria. Ann Med [24]
Health Sci Res. 7: pp.60-66
-
[13] Siddiqui AH, Raza SA, Ghazipura A, Hussain MA, Iqbal S, Ahsan K, et al. 2016.
Analysis of Association Between Type of
Amblyopia and Gender at a Tertiary Care [25]
Hospital in Karachi. Vol.66; No.5
-
[14] Rouse MW, Cooper JS, Cotter SA, Press LJ, and Tannen BM. 2004. Optometric Clinical Practice Guideline: Care of the Patient with Amblyopia. American Optometric Association, Lindbergh Blvd., St. Louis. [26]
-
[15] Yen KG, Roy H. 2016. Amblyopia; Pathophysiology. Department of Ophthalmology Cullen Eye Institute, Baylor College of Medicine. Tersedia pada: http://emedicine.medscape.com/article/1214 [27]
603-overview#a6. [diunduh 28 Desember 2016]
-
[16] Chua B, dan Mitchell P. 2004.
Consequences of amblyopia on education, occupation, and long term vision loss. Br J [28]
Ophthalmol; 88: pp.1119–1121.
-
[17] Carlton J dan Kaltenthaler E. 2011.
Amblyopia and quality of life: a systematic review. Eye 25: pp.403–413 [29]
-
[18] Basyir I, Arintawati P, dan Saktini F. 2016.
Perbedaan Penglihatan Stereoskopis pada
Penderita Anisometropia Ringan-Sedang dan Berat. Jurnal Kedokteral Diponegoro. [30] Vol.5.No.4: pp.1092-1100
-
[19] Barrett BT, Bradley A, dan Candy TR.
2013. The Relationship between
Anisometropia and Amblyopia. Prog Retin[31]
Eye Res. 36: pp.120–158
-
[20] Robaei D, Rose KA, Ojaimi E, Kifley A,
children. Archives of Ophthalmology. 124(6): pp.878–884.
Amblyopia among Junior High School
Students. Department of Ophthalmology, Faculty of Medicine, Gadjah Mada
University. Ophthalmol Ina; 41(3): pp.283288
Chia A, Dirani M, Chan YH, Gazzard G, Au Eong KG, Selvaraj P, et al. 2010.
Prevalence of amblyopia and strabismus in young Singaporean Chinese children.
Investigative Ophthalmology & Visual Science. 51: pp.3411–3417.
Faghihi M, Ostadimoghaddam H, dan Yekta AA. 2011. Amblyopia and strabismus in Iranian schoolchildren, Mashhad.
Strabismus. 19(4): pp.147–152
Pai AS, Rose KA, Leone JF, Sharbini S, Burlutsky G, Varma R, et al. 2012.
Amblyopia prevalence and risk factors in Australian preschool children.
Ophthalmology. 119(1): pp.138–144.
Gupta M, Rana SK, Mittal SK, dan Sinha RNP. 2016. Profile of Amblyopia in School going (5-15 years) Children at State Level Referral Hospital in Uttarakhand. Journal of Clinical and Diagnostic Research. Vol-10(11)
Sapkota K , Pirouzian A, dan Matta NS. 2013. Prevalence of amblyopia and patterns of refractive error in the amblyopic children of a tertiary eye care center of Nepal. Nepal J Ophthalmol;5(9): pp.38-44
The Pediatric Eye Disease Investigator Group. 2002. The Clinical Profile of Moderate Amblyopia in Children Younger than 7 Years. Arch Ophthalmol. 120: pp.281-287
Waris A, Amitava AK, NaheedAkhtar, Malakar M, dan Kritima. 2013. Amount of Anisometropia and Degreeof Amblyopia, a Correlation. UJO. Vol.8.No.1
Bhandari G, Byanju R, dan Kandel RP. 2015. Prevalence and Profile of Amblyopia in Children at Bharatpur Eye Hospital. Ann Pediatr Child Health 3 (8):1085
Smith EL, Hung LF, dan Harwerth RS. 2000. The Degree of Image Degradation and the Depth of Amblyopia. Invest Ophthalmol Vis Sci. 41(12): pp.3775–3781
Marthala H, Kamath G, Kamath M, dan Kamath SJ. 2017. Clinical Profile of Amblyopia in a Tertiary Care Teaching Hospital in Southern India. Indian J Ophthalmol. 65: pp.285-9
Repka MX, Simons K, dan Kraker R. 2010. Laterality of Amblyopia. American Journal of Ophthalmology. 150(2): pp.270–274.
Goh PP, Abqariyah Y, Pokharel GP, dan Ellwein LB. 2005. Refractive error and visual impairment in schoolage children in
Gombak District, Malaysia. Ophthalmology. 112(4): pp.678–685.
-
[34] Tarczy-Hornoch K, Varma R, Cotter SA, McKean-Cowdin R, Lin JH, Borchert MS, et al. 2011. Risk Factors for Decreased Visual Acuity in Preschool Children: The Multi-Ethnic Pediatric Eye Disease and Baltimore Pediatric Eye Disease Studies. Ophthalmology. 118(11): pp.2262–2273.
-
[35] Bacal DA, Miller AM, Kozak A, Feldman BH, Adamopoulou C, dan Epley KD. 2014. American Academy of Ophthalmology: Amblyopia. Tersedia pada: http://eyewiki.aao.org/Amblyopia. [diunduh 10 November 2017]
-
[36] Gunawan W. 2006. Astigmatisma Miop Simplek yang Mengalami Ambliopia pada Anak Sekolah Dasar di Yogyakarta. Berita Kedokteran Masyarakat Vol.22.No.3: pp.135-139
-
[37] Pramadani SF. 2015. Anisometropia. tersedia pada: https://www.scribd.com/doc/204907592/Ani sometropia. [diunduh 28 Desember 2016]
-
[38] Vidyapati. 1991. Kelainan Refraksi pada Anak-anak. Seminar Penyakit Mata, Muktamar XXI IDI: pp.13-21
-
[39] Brown SA, Weih LM, Fu CL, Dimitrov P, Taylor HR, dan McCarty CA. 2000. Prevalence of amblyopia and associated refractive errors in an adult population in Victoria, Australia. Ophthalmic Epidemiol 7 (4): pp.249-258
-
[40] De Zarate BR, dan Tejedor J. 2007. Current concepts in the management of amblyopia. Clinical Ophthalmology. 1(4) pp.403–414
-
[41] Hennesey CC. 2007. Anisometropic Amblyopia: Nonsurgical Treatment. Board of Regents of the University of Wisconsin System, American Orthoptic Journal; Volume 57
-
[42] Wallace D, Chandler DL, Beck RW, Arnold RW, Bacal DA, Birch EE, et al. 2007. Treatment of Bilateral Refractive Amblyopia in Children 3 to <10 Years Old. Am J Ophthalmol. 144(4): pp.487-496
-
[43] Stewart CE, Moseley MJ, Stephens DA, et al. 2004. Treatment Dose-Response in Amblyopia Therapy: The Monitored Occlusion Treatment Of Amblyopia Study (MOTAS). Invest Ophthalmol Vis Sci, 45: pp.3048–54
28
Discussion and feedback