Unilateral Usual Ductal Hyperplasia in A 22 Years Old Male Patient: A Case Report
on
DIRECTORY OF
OPEN ACCESS
JOURNALS


Unilateral Usual Ductal Hyperplasia in A 22 Years Old Male Patient: A Case
Report
Kelvin Setiawan1*, Bramastha Aires Rosadi1, Terry Renata Lawanto1, Primariadewi
Rustamadji2
1Department of Surgery, Tebet General Hospital, Jakarta Selatan, Indonesia.
2Department of Pathological Anatomy, Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
*Corresponding author: kelvin.setiawan.a@gmail.com.
ABSTRACT
Background: Benign breast disease have been broadly classified into non-proliferative lesions, proliferative lesions without atypia and hyperplasia with atypia. Proliferative disease, such as usual ductal hyperplasia, is associated with a 1.5 to 2 fold increased risk of developing invasive carcinoma. We reported a case of usual ductal hyperplasia in a young male. Case: A 22-year-old male complained of discomfort and enlargement of unilateral breast. Physical examination at that time revealed a palpable mass in the lateral upper quadrant of the patient’s left breast, three centimeters from nipple areola complex. The examination of axilla didn’t reveal any lymph node enlargement on both sides. His vital signs were normal without any abnormalities found on examination. Ultrasonography examination demonstrated fibroglandular tissue in the left breast with the volume of 11.13 cm3, consist of 4.8 cm length, 2.9 cm width and 0.8 cm depth. Excisional tumor biopsy was done on his left breast. Usual duct cell hyperplasia was present in microscopic examination with chronic inflammatory cells spreading around the fibrotic stromal cell. Physical examination, radiologic examination, and biopsy were all performed in this patient. Although the accuracy of the triple test is high, benign concordant results do not obviate further surveillance of a palpable mass. We advised our patient to routinely follow-up his condition every 6 months for 1 to 2 years, especially if there any changes found on his breasts. Conclusion: Any guidelines and further studies regarding patient’s follow-up examination after biopsy for male breasts tumor are needed in order of better understanding about this disease.
Keywords: usual ductal hyperplasia, male breast tumor, breast conserving surgery, triple test evaluation.
DOI: https://doi.org/10.24843/JBN.2019.v03.i02.p03
INTRODUCTION
Benign breast disease encompasses a wide variety of histological entities, which have been broadly classified as non-proliferative lesions, proliferative lesions without atypia, and hyperplasia with atypia. Nonproliferative lesions, as defined by Dupont and Page include cysts, changes in papillary apocrine, epithelial-related calcifications, and mild hyperplasia of the usual type. Included within the group of proliferative lesions without atypia are usual ductal hyperplasia (also known as moderate or florid hyperplasia
of the usual type), intraductal papilloma, sclerosing adenosis, and radial scars. Atypical hyperplasia has been defined as a proliferative lesion of the breast which gives rise to several features of carcinoma in situ and is classified as a ductal or lobular type.1
Epidemiologic studies have established the association of benign histological changes with the later development of invasive cancer. Proliferative disease, such as usual ductal hyperplasia, is associated with a 1.5 to 2 fold increased risk of developing invasive carcinoma.2 We report a case of usual ductal
41 | JBN (Jurnal Bedah Nasional)
hyperplasia in the male breast with the chief complaint of discomfort and enlargement of unilateral breast. Excisional biopsy was done, and biopsy results showed usual ductal hyperplasia.
CASE REPORT
The patient is a 22-year-old Asian male who reported a history of breast enlargement and pain on his left breast. He noticed an enlargement on his breast in the past seven years ago. He did not seek medical assistance at the time. The patient did not feel any pain until one month before first admission into Tebet general hospital. The pain was slightly dull and limited only around the tumor. Breast pain was intermittent and did not reside at rest. The patient did not have any history of alcohol consumption, smoking, and other conditions, such as diabetes mellitus, hypertension, and chronic diseases. None of the patient’s family members had a similar complaint and had no history of familial or genetic disorders.
Visually, the patient’s breasts looked symmetric without any pathologic signs. The skin around the tumor and breast were normal without any inflammation signs and satellite nodules. Nipple discharges were not found and nipples were not retracted at both sides. There were no other malignant signs such as dumpling of the breasts and peau d’ orange. Physical examination at that time revealed a palpable mass in the lateral upper quadrant of the patient’s left breast, three centimeters from nipple areola complex. The tumor was superficial and painless at the time of examination. The tumor was mobile and wasn’t fixed to any adjacent structure below the skin. The examination of axilla did not reveal any lymph node enlargement on both sides. His vital signs were a temperature of 36.3o C, a heart rate of 93 beats per minute, oxygen saturation of 98% and blood pressure
of 120/80 mmHg. His body mass index was 26.1 kg/m2. His weight was 81 kg and 176 cm height tall.
He was examined for breast ultrasonography. The examination demonstrated fibroglandular tissue in the left breast with the volume of 11.13 cm3, consist of 4.8 cm length, 2.9 cm width and 0.8 cm depth. Right breast appeared to be normal with no enlargement found. Both left and right axilla were normal with no enlargement lymph nodes found.

Figure 1. Ultrasonography Examination Result on Patient’s Left Breast
The patient underwent a surgical procedure for tumor biopsy. Excisional tumor biopsy was done on his left breast through circumareolar incision. The tissue was sent for pathological evaluations. The breast tumor specimen was approximately 4x2x1 cm3 in size, with a yellowish color and soft-elastic consistency. Microscopic examination revealed fibrous tissue, adipose tissue, and breast tissue, consisting of ductal covered with epithelial and myoepithelial cells. Usual duct cell hyperplasia was present in
microscopic examination with chronic inflammatory cells spreading around the fibrotic stromal cell. After ruling out the possibility of malignant breast mass, the patient was advised to follow-up his condition every 6 months for 1 to 2 years.
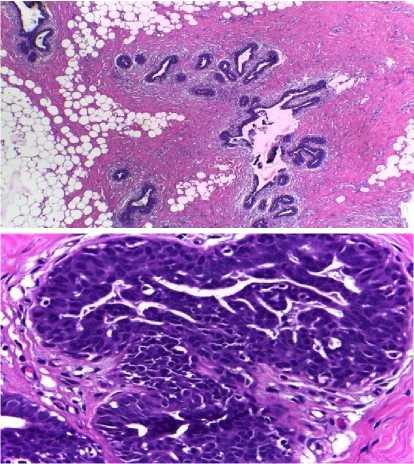
Figure 2. Histopathology Result from Patient’s Left Breast after Excisional Biopsy
DISCUSSION
Usual ductal hyperplasia (UDH) is intraductal epithelial proliferation more than four epithelial cells. They are characterized by a tendency to bridge and often distend the involved space. The proliferation may have a solid, fenestrated or papillary architecture. If spaces remain within the duct lumen, they are irregular and variable in shape. These spaces are often slit-like and arranged around the periphery of the proliferation, with their long axes parallel to the basement membrane. The cells comprising this type of proliferation are cytologically benign and variable in size, shape, and orientation, and they often are arranged in a “swirling pattern. It is sometimes possible to discern multiple distinct cell populations, including epithelial cells, metaplastic apocrine cells, and myoepithelial cells.1
In Oren Lapid et al. analysis of 5113 gynecomastia breasts, the average age of the patients was 35.8 ± 18.3 years (range, 1-88 years). Most interventions (1809 interventions, 48.5%) were performed in the age groups of 10 to 19 and 20 to 29 years; with increasing age, the number of interventions decreased. From histology examinations, Oren et al. found nine patients with unilateral atypical ductal hyperplasia. One patient unilateral atypical ductal hyperplasia was found in 20-29 age groups. In our case report, the patient was 22 years old with the unilateral painless mass on his left breast.3 We could not find any data regarding usual ductal hyperplasia in male breast, their case prevalence, and their histology results. We hope in the future, data concerning UDH in a male patient from descriptive studies or case reports will be more available.
Masses that are found to be solid on imaging require triple-test evaluation which refers to physical examination, radiologic examination, and needle biopsy performed by core or fine-needle aspiration (FNA). The triple test is performed even in cases where masses are considered benign on imaging because some malignant lesions can have a benign appearance.1 The surgical excision of a lesion in the breast with the intent to remove it entirely is referred to as an excisional biopsy4, which was done to the patient. Physical examination, radiologic examination, and biopsy were all performed in this patient.
Although the accuracy of the triple test is high, benign results do not exclude further surveillance of a palpable mass. Serial examinations and imaging at six months intervals for 1 to 2 years are recommended. We advised our patient to routinely follow-up his condition, especially if there any changes found on his breasts. We could not find any
guidelines regarding patient’s follow-up examination after biopsy for male breasts tumor, particularly UDH. Therefore, it needs further upcoming reports and research in order of better understanding of this disease.
Benign breast disease encompasses a wide variety of histologic entities, which have been broadly classified into non-proliferative lesions, proliferative lesions without atypia, and hyperplasia with atypia. With the increased use of mammography, more benign lesions are being detected, and accurately estimating the risk of breast cancer for specific histologic categories is of great importance to guide clinical management. Included within the group of proliferative lesions without atypia are usual ductal hyperplasia (also known as moderate or florid hyperplasia of the usual type), intraductal papilloma, sclerosing adenosis, and radial scars. Proliferative disease, such as usual ductal hyperplasia, is associated with a 1.5 to 2 fold increased risk of developing invasive carcinoma.1,2,5
CONCLUSION
The term Usual Ductal Hyperplasia (UDH) is now used to distinguish this lesion in its common and florid forms from Atypical Ductal Hyperplasia (ADH). The triple test is performed even in cases where masses are considered benign on imaging because some malignant lesions can have a benign appearance. Limited evidence concerning UDH in male patients, including prevalence,
clinical presentation and management aspect, hopefully encourages for upcoming descriptive studies and guidelines regarding UDH in male patients.
ACKNOWLEDGEMENT
None.
DISCLOSURE
Authors declare no conflict of interest of this report.
REFERENCES
-
1. Harris JR, Lippman ME, Morrow M, Osborne CK. Diseases of the breast, 5th edition. Philadelphia: Lippincott
Williams and Wilkins; 2014. p.71-73.
-
2. Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease, 9th edition. Philadelphia: Elsevier
Saunders; 2014. p. 1048-51.
-
3. Lapid O, Jolink F, Meijer SL. Pathological findings in gynecomastia analysis of 5113 breasts. Ann Plast Surg. 2015;74:163-6.
-
4. Johnson RE, Kermott CA, Murad MH. Gynecomastia - evaluation and current treatment options. Ther Clin Risk Manag. 2011;7:145-8.
-
5. Kabat GC, Jones JG, Olson N, et al. A multi-center prospective cohort study of benign breast disease and risk of subsequent breast cancer. Cancer Causes Control. 2010;21:821-8.
44
Discussion and feedback