Bochdalek Hernia
on
CASE REPORT
BOCHDALEK HERNIA
Yuliaji Narendra Putra1, Tubagus Odih Rhomdani Wahid2, Guntur Surya Alam2, Rohadi3
-
1General Surgery Training Programme, Faculty of Medicine Gadjah Mada University, Dr. Sardjito Hospital. Correspondence: yp_narendra@yahoo.com.
-
2Pediatric Surgery Training Programme, Faculty of Medicine Gadjah Mada University, Dr. Sardjito Hospital. 3Pediatric Surgery Division, Faculty of Medicine Gadjah Mada University, Dr. Sardjito Hospital.
ABSTRACT
Background: Bochdalek hernia is a congenital defect on posterolateral diaphragm with an abnormal connection between the thoracic cavity and the abdominal cavity. This disease causes protrusion of abdominal organs into the thoracic cavity. Case: an 8-day-old baby girl admitted to hospital with shortness of breath 24 hours after delivered. The baby was born spontaneously assisted by midwife. Upon born, the baby was crying strongly and meconium came out 2 hours after birth. On physical examination, the abdomen was inspected flat. Darm contour and darm steifung was observed, and peristaltic sound was heard on left lung. Radiological examination demonstrated a diaphragmatic hernia with ileus obstruction. The patient underwent laparatomy and stomach, ileum, transverse colon, and spleen, was found on foramen Bochdalek. Post-surgery chest X Ray showed favourable result. Ten days after treatment, the patient was discharged in a good condition with no respiratory or digestive problems. After 1 months the patient’s condition remained good and there were no respiratory or digestive complaints. Conclusion: In a rare case like Bochadalek hernia, laparotomy performed as a promising attempt to return the anatomic position of organ.
Keywords: Bochdalek hernia, laparotomy, surgery.
HERNIA BOCHDALEK
Yuliaji Narendra Putra1, Tubagus Odih Rhomdani Wahid2, Guntur Surya Alam2, Rohadi3
-
1Program Studi Ilmu Bedah, Fakultas Kedokteran Universitas Gadjah Mada, RSUP Dr. Sardjito. Korespondensi: yp_narendra@yahoo.com.
-
2Program Studi Ilmu Bedah Anak, Fakultas Kedokteran Universitas Gadjah Mada, RSUP Dr. Sardjito. 3Divisi Bedah Anak, Fakultas Kedokteran Universitas Gadjah Mada, RSUP Dr. Sardjito.
ABSTRAK
Latar belakang: hernia Bochdalek adalah cacat bawaan pada diafragma posterolateral yang terdapat hubungan antara rongga thoraks dan rongga perut, sehingga terjadi penonjolan organ perut ke dalam rongga thoraks. Kasus: seorang bayi perempuan umur 8 hari dibawa ke rumah sakit swasta dengan keluhan sesak nafas 24 jam setelah dilahirkan. Satu minggu yang lalu, pasien lahir spontan ditolong bidan,menangis kuat, mekonium keluar 2 jam setelah lahir. Pada pemeriksaan fisik didapatkan abdomen flat,didapatkan darm contour dan darm steifung, Suara peristaltik terdapat pada auskultasi di hemithoraks kiri. Pada pemeriksaan radiologis terdapat gambaran udara usus pada hemithoraks kiri. Dari pemeriksaan diatas ditegakkan diagnosis hernia diafragmatika dengan ileus obstruksi. Dilakukan laparotomi, durante operasi didapatkan gaster, ileum, kolon transversum, dan lien masuk ke dalam rongga thoraks sinistra, defek ukuran 2x8 cm pada posterior (foramen Bochdalek). Rontgen thoraks post laparotomy paru-paru mengembang kedua sisi dan diafragma kiri terlihat intak. Sepuluh hari setelah menjalani perawatan, pasien pulang dengan keadaan baik tidak ada gangguan pernafasan maupun pencernaan. Evaluasi selama 1 bulan terkhir keadaan pasien tetap baik
dan tidak ada keluhan pernafasan maupun pencernaan. Simpulan: telah dilakukan laparotomi untuk mengembalikan ke posisi anatomi pada pasien hernia Bochdalek dengan hasil baik.
Kata kunci: hernia Bochdalek, laparotomi, operasi.
INTRODUCTION
Bochdalek hernia is a congenital defect on posterolateral diaphragm with an abnormal connection between the thoracic cavity and the abdominal cavity, resulting in the protrusion of the abdominal organs into the thoracic cavity.1 The incidence in neonates is 1:2000-50002-3 with pulmonary hypoplasia as the most common complication.4 Despite advances in the diagnosis and treatment of congenital defects, pulmonary hypoplasia still caused a fairly high mortality rate.5,6
Surgical treatment can be performed either through the abdominal or thoracic approach. The abdominal approach has the advantage of correcting malrotation at the same time.7 However, closure of the abdominal wall can result in the difficulty of organs replacement to abdominal cavity. For the solution, Charles et al has recommended a delayed abdominal muscle closure. In this case, it will be presented regarding the management of Bochdalek hernia in children.
CASE REPORT
An 8-day-old baby girl was admitted taken to a private hospital with shortness of breath. The patient was born spontaneously assisted by midwife, crying strongly, and meconium came out 2 hours after birth. At 24 hours later, the patient appeared to have difficulty of breathing, and referred to a primary hospital. After 6 days of treatment, no improvement was observed, thus the patient was referred to a tertiary hospital.
In physical examination, the baby showed high body temperature, shortness of breath with respiratory rates 39 times per minute, but the baby could cry strongly. Chest x-ray examination showed multiple cystic shadow at the left hemithorax accompanied by right deviation of mediastinum and trachea with suspicion of diaphragmatic hernia. On the abdominal x-ray, the distal end of the nasogastric tube only reached 5th-6th thoracic vertebra with intestinal air portrayed on the left chest. Babygram examination showed that left intestine on hemithorax was unfilled with contrasts, the air intestinal image on the left hemithorax is not filled with contrasts, with left diaphragmatic hernia image showing intestines and colon (Figure 1).

Figure 1. Babygram pre-surgery.
Preoperative diagnosis is left diaphragmatic hernia and laparotomy surgery via abdominal approach was decided. A transverse incision of the upper umbilical (3 cm above of umbilicus), deepened layer by layer to the peritoneum. After the peritoneum was opened,
intestinal, gastric, and part of transverse colon system were seen inside of the abdomen. The inlet of foramen Bochdalek was seen released and re-inserted the content of the hernia consisting ileum and part of colon to the inside of the abdomen cavity (Figure 2). The diameter of foramen Bochdalek was 2x8 cm, then incision on septum tendinous was made then 2 layers was sutured. Aspiration of pleura cavity was performed with nasogastric tube. Exploration showing intestinal systems is intact. The surgical wound was closed layer by layer. The surgery was completed.

Figure 2. Clinical picture during surgery.
Chest X-ray after surgery showed inflation of left lung. The patient was treated for 10 days and discharged on the 11th day after the surgery. Follow up for 1 months shows patient’s good condition and neither disturbance was observed in the digestive system nor respiratory system.
DISCUSSION
Bochdalek hernia (Figure 3) is a congenital defect on posterolateral diaphragm developing an abnormal connection between the thoracic cavity and the abdominal cavity. This pleuroparietal canal normally closed by the pleuroparietal membrane at the 8th to 10th week of
pregnancy. Failure of canal closure might result in Bochdalek hernia. Approximately 80-90% cases of Bochdalek hernia occur on the left side and are very rare in adults. In this case, a large defect in the left posterolateral diaphragm (Bochdalek foramina) was encountered with the content of ileum and part of colon.4,5 Bochdalek hernia diagnosed from anamnesis, physical examination, investigation especially chest x-ray and OMD.6
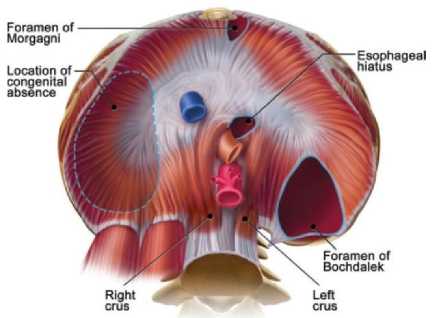
Figure 3. Location of Bochdalek Foramen.8
The diagnosis of this patient was made after physical and radiological examination because rarity of this disease and the nonspecific diagnosis could lead to delay of diagnosis. Surgical repair of the defect is the recommended therapy for Bochdalek Hernia.7 For this patient, laparotomy surgery was performed with abdominal approach.8 A transverse incision of the upper umbilical (3 cm above of umbilicus), deepened layer by layer to the peritoneum. After the peritoneum was opened, intestinal system, gastric, and part of transverse colon was seen inside of the abdomen. Post-surgery showed inflation of left lung. Long term follows up was also favourable. This showed that laparotomy for management of Bochdalek Hernia led to either short term and long term results.
CONCLUSION
Laparotomy performed as an attempt to return the anatomic position of patient with Bochdalek hernia showing good result.
REFERENCES
-
1. Brunicardi FC, Billiar TR, Dunn DL, et al. Congenital Diaphragmatic Hernia. In: Schwartz SI, Fischer JE, Daly JM, et al., editors. Schwartz’s Principles of Surgery. 7th Edition.
Asian Student Edition. Singapore: McGraw-Hill; 1998. p.1691-3.
-
2. Way LW. Esophagus & Diaphragm. In: Way LW, Doherty GM, editors. Current Surgical Diagnosis and Treatment. 11th Edition. Connecticut: McGraw-Hill/Appleton & Lange; 2002. p.438-40.
-
3. Townsend CM, Beauchamp RD, Mattox KL, et al. Congenital Diaphragmatic Hernia In: Townsend CM, Beauchamp RD, Evers BM, et al., editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 16th Edition.
Philadelphia: WB Saunders; 2001.
p.1480-3.
-
4. Eisenberg RL. Esophagus and Diaphragmatic Hernia In: Eisenberg RL, editor. Diagnostic Imaging in Surgery. New York: McGraw-Hill; 1987. p.275-6.
-
5. Liechty RD. Respiratory
Diaphragmatic Hernia. In: Niederhuber JE, editor. Fundamentals of Surgery. Stamford: Appleton & Lange; 1998. p.192-3.
-
6. Reynolds M. Diaphragmatic
Anomalies. In: Raffensperger JG, editor. Swenson’s Textbook of Paediatric Surgery. 5th edition. New
York: Appleton & Lange; 1990. p. 721-30.
-
7. Burki T, Amanullah A, Rehman AU, et al. Late Presentation of Bochdalek Hernia with Intestinal Symptoms. J Ayub Med Coll Abbottabad. 2002;14: 27-8.
-
8. Nason LK, Walker CM, McNeeley MF, et al. Imaging of the Diaphragm: Anatomy and Function.
RadioGraphics. 2012;32:E51-70.
43
Discussion and feedback